
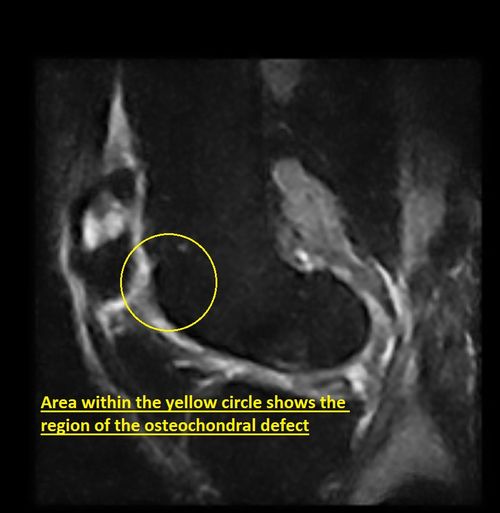
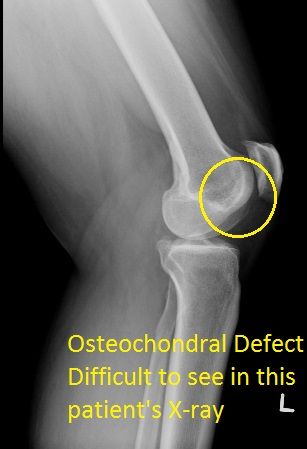
Ms. C.G. a 37 year old female, a waitress by profession, presented with left knee pain for a few months. She had had no past trauma to the affected area. She states that she has discomfort while “walking up and down stairs”. On physical examination by one of our experienced Orthopaedic consultants, it was found that Miss C.G. had a limp in the left knee, incomplete flexion and extension and she experienced pain on attempting to move the knee joint. She had no swelling and her X-rays showed minimal degenerative changes. She was referred for an MRI of her left knee, which showed a medial meniscal tear and a lateral patellar tilt and patella alta(high patella), which resulted in a lateral patellar facet osteochondral defect and patello-femoral osteoarthritis.
Ms. C.G. was advised on the need for surgery. It was mutually agreed that an arthroscopy of her left knee with debridement be performed. At surgery, findings included an osteochondral lesion of the lateral tibial plateau that was cleaned, a medial meniscal tear that was debrided back to stability and the osteochondral grade II-III wear of the patella debrided and stabilized.
Miss C.G. at 3 months post operatively, despite participating in routine physiotherapy, had issues with descending slopes or stairs where she would experience pain behind the knee cap while performing these actions. At 5 months post op, after monitoring the pain, the decision was taken to inject her left knee joint with Synvisc (an injection that supplements the fluid in the knee to help lubricate and cusion the joint). The Synvisc injection helped minimally as she still experienced pain and swelling while descending stairs. X-rays of the left knee showed a continuing retropatellar osteochondral defect. She had a second MRI which showed an improvement in the lateral patellar facet osteochondral defect (most likely due to the conservative treatment). She had a repeat Synvisc injection, however the pain persisted and eventually discussed the need for a second surgery.
Her second surgery consisted of medial meniscal repair and debridement of her osteochondral lesion. Approximately 13 weeks after her second surgery, she lost weight and her symptoms improved, however still managed to get pain after long activities.She was then advised on the need for an OATS (Osteochondral Autograft Transfer System) procedure. This is a procedure that involves cartilage and bone transfer from the area of the knee that is healthy to a damaged area of the knee. In this case , an allograft was used (a tissue graft from a DONOR.) The OATS procedure was done and she is yet to be followed up.
Posted:

Posted:
Posted: