A 29 year old male was seen for consultation in August of 2013. He is a Semi-Professional footballer and also works with the Coast Guard. He has been having right knee pain and swelling for 2 years. In addition to this, he has also had episodes of his right knee "giving out". His symptoms progressed with time, when eventually, he had begun to experience marked difficulty with performing daily activities. The progression of his pain eventually led to him having to make the decision to stop playing football. This patient was initially seen at another institution and was recommended for an arthroscopy (internal camera inspection of the knee joint), lateral meniscal repair and an Anterior Cruciate Ligament reconstruction.
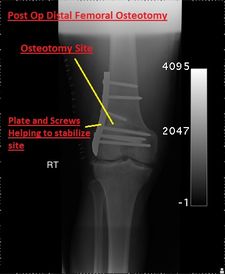
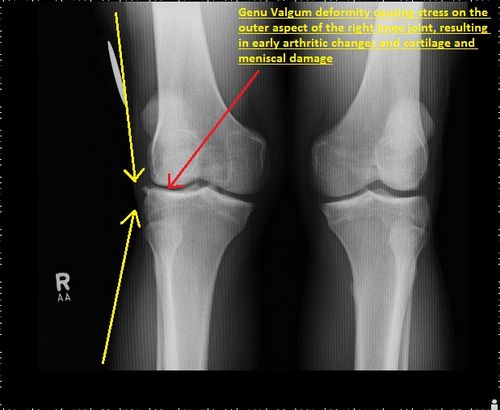
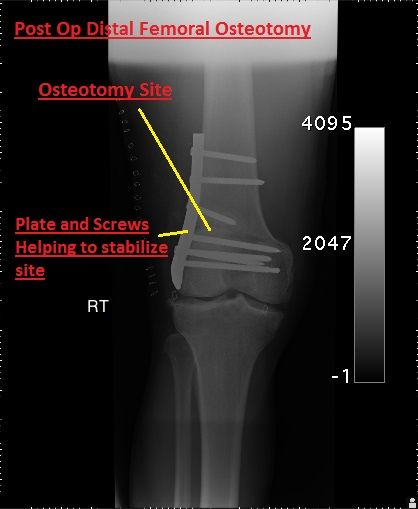
On clinical examination at The Fracture and Orthopaedic Clinic, the right knee revealed a genu valgum deformity (the opposite of a bow leg deformity, so the knees are pushed inwards). He has no instability of his knee joint in any plane however has marked tenderness in the outer aspect of his knee joint. His X-rays showed significant joint space narrowing and early arthritic changes in his knee. His MRI scan showed significant cartilage damage nearing to bone, as well as a tear in his lateral meniscus (the cushion of the knee). All of these degenerative changes are occurring because of his genu valgum deformity (shown in X-ray below). Therefore correction of this deformity is the main goal behind his treatment, or else his knee would have continued to deteriorate. A corrective distal femoral osteotomy was decided upon to re-align the knee joint.
3 months after his procedure he has almost full range of motion of his right knee and his alignment appears neutral. About one year later, he has improved significantly and is now in the gym doing cycling. 2 years post op, he had his implants removed, and is now being rehabilitated to regain normal activities.
Posted:
Posted:

Posted: