
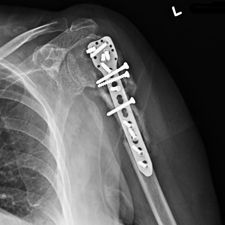
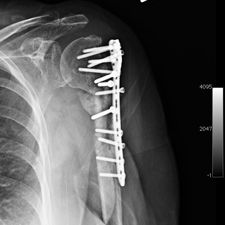
Ms. Q, age 74, initially presented on December 10, 2009, following a multiply comminuted, osteoporotic fracture of her left proximal Humerus. The decision was made to do an ORIF, which was carried out on December 14, 2009. She had a locking plate implanted following which she developed an infection of the wound. She was initially treated with antibiotics for this and she continued to get some oozing of the wound, which did not settle down despite continued use of the various antibiotics including Augmentin. Multiple wound swabs were done which failed to grow any organisms. The oozing persisted until about eight weeks following her operation when it finally settled down and the scar was noted to be tethered and was thought to be tethered onto bone.
She continued to have problems with intermittent cellulitis and pain in the arm and the decision was made to do an early removal of the metal work. This was carried out in mid March 2010 and at operation, which was done through the original incision and anterior extended deltopectoral approach, she was noted to have healed the fracture. She did well postop and was continuing to mobilize.
Some time in late May 2010, she presented with movement of the fracture site and was noted that the central area of healing had broken down and was thought that she had a deep infection. She was taken back to theater in mid June 2010 when operation showed that there was no pus. Multiple samples of the fracture site were taken and an external fixator applied with compression of the fragments. Following that, the cultures taken from the wounds showed no growth and no organisms and a biopsy showed no sign of any malignancy or abnormal cells. The fixator became loose and eventually had to be removed. This was done in July 2010 and she was discovered to be going onto a hypertrophic nonunion. Low dose ultrasound treatment of the fracture site was tried to help stimulate healing over the course of a few months but the non union persisted.
She was advised of the need to do some sort of stabilization which is necessary since the use of low-dose ultrasound has not helped in the healing process. She was unwilling to have any further operative intervention and sought further options. Eventually, she agreed to a fourth procedure of intra-medullary nail stabilization of the fracture and had this carried out in April 2011. An intramedullary nail was inserted in an antegrade manner and she has since gone on to heal the fracture site completely and has regained most of the function of the upper limb with no pain.
This case illustrates the possible complications that can occur with any surgery but also our commitment to our patients by sticking with them and making sure that a positive outcome is had despite the many challenges that may arise.

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015

Posted: Dec 1, 2015
Posted: Dec 1, 2015
Posted: Dec 1, 2015

Posted: Dec 1, 2015